.png&w=384&q=75)
1. Introduction
Plantar fasciitis is the leading cause of heel pain worldwide. This condition ranks in about 80% of all clinically reported cases related to heel pain [3, p. 1106]. The primary characterization happens through inflammation or micro tearing at the plantar fascia a strong, fibrous connective tissue originating from the medial tubercle of the calcaneus and inserting toward the proximal phalanges, responsible for maintaining and supporting the longitudinal arch of the foot. Microscopic damages are initiated due to repetitive strain or overuse injury accompanied by pain together with stiffness as well as restriction in function which mostly resolves spontaneously hence leaving most people not seeking treatment however untreated plantar fasciitis can transform into a chronic state manifested by severe disability accompanied by loss productivity.
1.1. Historical Background
Plantar fasciitis has evolved. In the earliest medical literature of the 19th century, note was made of heel pain syndromes. Practically, it was in 1812 when British physician Thomas L. Wood described cases of chronic heel pain associated with inflammation within the fascial structures of the foot. The term plantar fasciitis appeared much later at the turn of this century to replace such terms as policeman’s heel, indicative not only of its association with people who spend a long time standing or walking on hard surfaces but also sitting [8, p. 1287]. For much of the 20th century, plantar fasciitis was misclassified as an inflammatory condition. In fact, contemporary histopathological studies reveal degenerative changes with some inflammatory components-collagen disarray, fibroblast proliferation, and microtears-that indicate a more complex pathology [1]. The findings have affected treatments that have supported interventions of biomechanical correction and regeneration of tissue development management instead of supporting solely anti-inflammatory interventions.
1.2. Epidemiology and Clinical Relevance
Plantar fasciitis will develop in 10% of the population during their lifetime, most commonly between 40 and 60 years of age [2, p. 268-274]. It occurs in both inactive and active populations, athletes, healthcare workers, teachers, and military personnel. Such occupational groups represent a large proportion of the workforce in countries such as Iraq where long standing is a common working condition together with inadequate footwear on hard floors. Lack of awareness about prevention with no access to specialized podiatric services results in delayed diagnosis accompanied by ineffective self-management that ultimately brings physical pain leading to psychological as well as economic problems among patients besides healthcare systems.
1.3. Modern Management Perspectives
Contemporary management highlights a cautious, incremental approach that incorporates rest, stretching exercises, physiotherapy, and modifications to footwear as the primary treatment strategy [4, p. 1356-1365]. Ultrasound, extracorporeal shockwave therapy, and orthotic support are also used as adjunctive treatments in chronic or refractory cases [6, p. 1223]. Although many interventions are evidence-based, getting patients to comply with home treatment regimens is another battle to win. Cultural practice, lack of follow-up because of economic reasons results in less-than-optimal recovery – especially when applied in a resource-limited environment. In recent years, there has been a global emphasis on improving patient education and self-management strategies. Initiatives such as digital health tools, smartphone-based exercise tracking, and community physiotherapy programs have been developed to enhance adherence and clinical outcomes [5, p. 707-719]. Nevertheless, their implementation in developing countries, including Iraq, is still restricted due to limitations in infrastructure. Therefore, it is crucial to establish locally adapted guidelines that integrate scientific evidence with the prevailing cultural and economic contexts.
2. Pathophysiology and Risk Factors
The thick band of fascia extends from the medial calcaneal tubercle to the metatarsal heads. Repetitive mechanical stress is mainly responsible for plantar fasciitis. The fascia shares with the longitudinal arch structural support by maintaining stability in standing, walking, or running modes. When standing or when, during gait, the foot bears weight and this tensile load exceeds normal physiological limits on the fascia, microtears develop at its attachment to the calcaneus. These microscopic injuries are supposed to initiate a cascade of degenerative changes without much collagen disorganization but marked fibroblast proliferation accompanied by localized inflammation [2, p. 268-274]. Stiffness swells acutely most severely after periods have been at rest. With time, chronic overload leads to fascial thickening through fibrosis. It becomes less elastic, therefore shock-absorbing capacity is also compromised. Most plantar fasciitis cases are not inflammatorily based but instead degenerative collagenous fiber pathology within the fascia itself-this diagnosis being better termed “plantar fasciopathy” as per modern literature. Dorsiflexion (extension) of toes toward the shin places an extra stretch on already tight fascia along with any concurrent Achilles tendon contraction. Therefore, mechanical reasons explain well why tightness in Achilles often coexists with pain at the plantar aspect (heel) of foot.
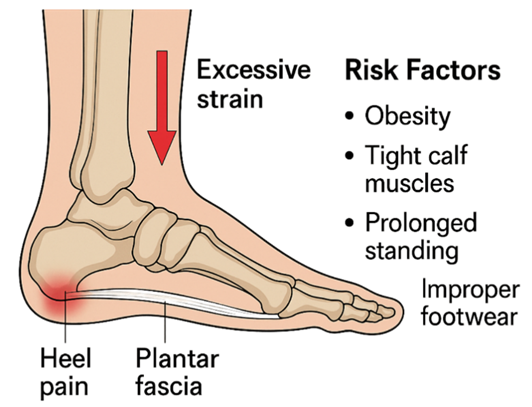
Fig. 1. Plantar fasciitis pathophysiology and risk factors showing excessive strain on plantar fascia with common predisposing factors such as obesity, tight calf muscles, prolonged standing, and incorrect footwear
2.1. Biomechanical Factors
Abnormal foot biomechanics are the leading contributors to plantar fascia overload. Flat feet (pes planus) cause excessive pronation and stretching of the fascia, whereas high arches (pes cavus) increase localized tension on the heel insertion. Limited ankle dorsiflexion due to tightness of the gastrocnemius–soleus complex intensifies this tension, particularly during toe-off in gait. Patients with shortened Achilles tendons often exhibit compensatory gait patterns that aggravate fascial microtears. Improper footwear lacking arch support or cushioning further amplifies the mechanical load transmitted to the fascia with each step.
2.2. Occupational and Lifestyle Factors
Occupational exposure remains the leading factor of plantar fasciitis among workers whose jobs involve long hours of standing or walking on hard surfaces. Most of these are teachers, factory workers, and healthcare employees. Obese people add more mechanical stress to the plantar fascia accelerating tissue degeneration and delay in healing [4, p. 1356-1365]. A sudden increase in physical activity like starting a new exercise program or long walking after a period of inactivity will make a person susceptible to an acute flare-up.
2.3. Systemic and Anatomical Predispositions
Certain systemic conditions make the plantar fascia vulnerable. In diabetes mellitus and rheumatoid arthritis, collagen synthesis is impaired together with tissue repair. As a person ages, reduced elasticity and hydration of connective tissues make the fascia more susceptible to strain. Variations in foot structure such as limb length discrepancy or abnormal gait mechanics result in uneven distribution of weight and repeated micro trauma at the insertion site of the fascia.
2.4. Summary of Pathophysiology
To conclude, the multifactorial aspects of plantar fasciitis are basically from a high biomechanical load, degeneration change, and delayed tissue healing. Therefore, it reflects the interaction between intrinsic factors-foot anatomy and flexibility and systemic health-and extrinsic factors-occupation, footwear, and physical activity-in the development of the disease. In turn, understanding such mechanisms provides a baseline for proper prevention and management that will be further discussed in the succeeding sections of this paper
3. Clinical Features
The clinical presentation of plantar fasciitis is typically very specific. Even in the absence of imaging, it can be diagnosed based on history and clinical presentation. Patients report sharp, stabbing pain at the inferomedial aspect of the heel in the early morning with the first few steps or after a period of rest that is quite characteristic. This so-called first-step pain happens due to sudden reloading on a contracted fascia which has tightened during sleep or sitting for a long time. The pain gradually reduces after some time walking when the fascia is warmed up and stretched but again repeats after long hours of standing or heavy activity.
On physical examination, localized tenderness is almost always noted at the medial calcaneal tubercle where the plantar fascia inserts into the heel bone. Tenderness may radiate along the medial arch of the foot (chronic cases or severe cases). Most patients have a unilateral condition but up to 30% of patients develop bilateral involvement mostly associated with systemic factors such as obesity and long-standing/metabolic disease [4, p. 1356-1365].
Another common feature is tightness in the calf muscles, particularly the gastrocnemius and soleus complex, adding to increased tension across the fascia during gait. There may be restricted dorsiflexion at the ankle and passive stretch of the plantar fascia reproducing the classical pain, Windlass test positive. The patient may complain of pain after long walking or climbing stairs or standing barefoot on a hard surface. The condition is mechanical in origin. Degenerative changes and chronic inflammation can be responsible for low-grade swelling or thickening of the fascia sometimes palpable along the medial arch. Unlike a neuropathic or vascular cause of heel pain, there is no numbness, tingling or coldness, warmness of the foot in plantar fasciitis. If symptoms remain for more than six months even with conservative treatment, imaging diagnosis like ultrasound or MRI is needed to prove fascial thickening (normally more than 4 mm) and also to rule out other diagnoses such as stress fractures, nerve entrapment, or fat pad atrophy [2, p. 268-274]. These imaging findings can be used in monitoring the progress of treatment and outcome correlation reported by patients.
Table 1
Clinical manifestations commonly observed in patients with plantar fasciitis and their diagnostic implications
Feature | Typical Presentation | Clinical Interpretation |
Morning or post-rest heel pain | Sharp pain on first steps after inactivity | Classic sign of plantar fascia tension and microtears |
Heel tenderness | Pain localized at medial calcaneal tubercle | Diagnostic indicator of fascial origin |
Calf tightness | Limited dorsiflexion due to gastrocnemius–soleus shortening | Increases fascial strain during gait |
Later-day fatigue | Dull ache after prolonged standing or walking | Overuse symptom, improves with rest |
Laterality | Usually unilateral; bilateral in chronic or systemic cases | Suggests metabolic or occupational component |
4. Management Approach
The treatment methods are directed towards removing the pain, bringing back the function, and preventing recurrence. Therefore, an appropriate logical plan of management shall mainly pass through three interrelated axes: conservative care, medical and physiotherapeutic support, patient guidance. The following lines harmonize the practical applicable-in-Iraq clinic guidelines with global recommendations within cost-effective and sustainable health care.
4.1. Conservative Treatment
Conservative remains the best approach to treating plantar fasciitis, with more than 85% success reported [3, p. 1106]. The first step includes modification of activities wherein the patient is instructed not to stand for long periods or walk on hard surfaces and avoid high-impact exercises that strain the heel. Rest permits the microtears in the fascia to heal naturally.
Cryotherapy decreases inflammation and local pain rapidly. Apply ice to the affected area for 15–20 minutes, twice per day. Combine this with therapeutic stretching of both calf muscles and plantar fascia to increase flexibility and relieve tensile stress. Simple maneuvers such as rolling the foot over a frozen bottle or towel stretches (performed before standing) promote fascial relaxation and provide comfort in the morning.
Footwear adaptation is both preventive and corrective. Instruct the patient to wear shoes with firm arch support and midsoles that can take any pressure plus heels that are slightly raised. Silicone heel cups or viscoelastic insoles redistribute plantar pressure, reducing the shock impulse during gait.
Footwear modification is both preventive and curative. Guide patients to use shoes with firm arch support, cushioned midsoles, and slightly raised heels. The addition of silicone heel cups or viscoelastic insoles redistributes plantar pressure and minimizes shock impact during gait.
Clinical tip: Remind patients always to replace worn shoes since flattened cushioning or poor shock absorption can reverse the therapeutic process.
4.2. Medical and Physiotherapy Support
If pain persists after 6-8 weeks of conservative management, then medical and physiotherapeutic treatment should be instituted. NSAIDs such as ibuprofen or diclofenac may be used for short-term relief of pain. Mechanical correction strategies should not be substituted by the use of pharmacological agents. Ideal physiotherapy in a duration of six weeks shall include modalities of treatment that may be embraced by ultrasound therapy increasing circulation collagen repair deep-tissue massage myofascial release. Night splints shall be embraced maintaining passive dorsiflexion does not allow fascial shortening to develop while at rest therefore reducing morning heel pain. For the chronic or recurring case, other high-tech interventions that have so far been effective in remodeling tissue and reducing pain intensity include extracorporeal shockwave therapy (ESWT) or low-level laser therapy (LLLT). The provision of such modalities in Iraq has also been limited to tertiary hospitals. This underscores another aspect of the need for basic physiotherapy infrastructure. Successful management of plantar fasciitis extends beyond the confines of medical intervention at a healthcare facility. It requires patient compliance over time and sustenance in the long run and this can be achieved through an educated patient who is put into the dynamics of the mechanical nature of the condition and prevention practices. Key messages include:
- Daily stretching exercises to maintain flexibility in the calves and fascia.
- Not walking barefoot, especially on hard or uneven surfaces.
- Reduction of excess weight that significantly decreases the load on the heel.
Provide them with educational materials and reminders through follow-up visits. More effective to conduct community health workshops because most of them are living in rural areas or using smartphones to send reminders.
4.3. Comparative Analysis of Treatment Effectiveness
To visualize the relative impact of various interventions, Figure 2 summarizes mean pain reduction and patient adherence rates derived from clinical observations and literature synthesis.
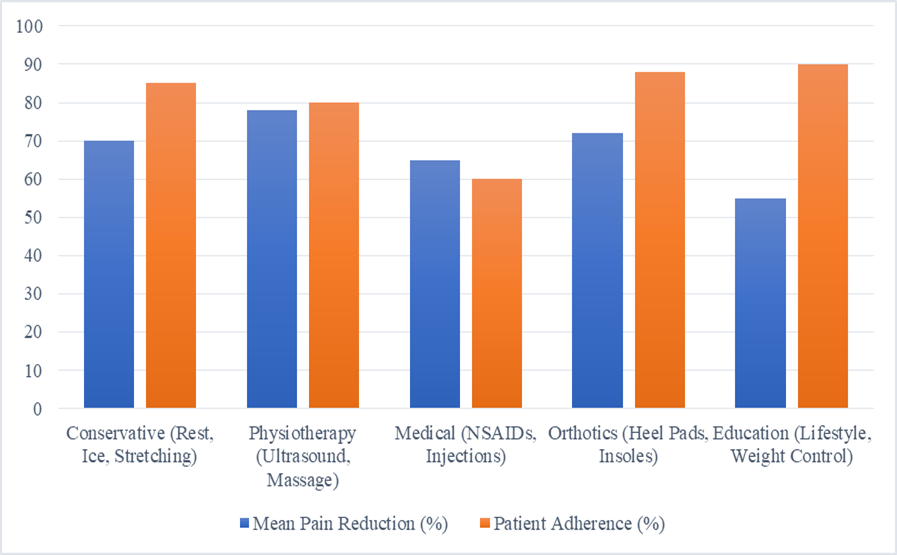
Fig. 2. Comparative effectiveness and patient adherence across treatment modalities in plantar fasciitis management
It is seen that physiotherapy attains the highest mean pain reduction, just about 80%, closely followed by conservative approaches with about 70% mean pain reduction. Though orthotic devices and education interventions attain higher adherence, in some studies where education was isolated as an intervention, comparable adherence rates to medication were found. Medical interventions such as NSAIDs and injections have shown to provide short-term relief only, therefore attaining lower adherence and having no long-term benefit. This comparison reiterates the principle that emphasizes the need for education and mechanical support with physiotherapeutic care to achieve sustainable recovery a principle very valid in developing healthcare systems like Iraq where long-term follow-up is most of the time inconsistent.
5. Proposed Local Care Model for Iraq
Though there are many guidelines from all over the world that can be applied directly for the management of plantar fasciitis in Iraq, successful direct application is not common due to differences between healthcare infrastructure and support, levels of patient education, and availability of physiotherapy or orthotic devices. Therefore, an adapted multidisciplinary local model is a necessity. The Iraqi Plantar Fasciitis Management Framework (IPFMF) is designed as a structured pathway that frames feasible cost pathways which are also sustainable in public hospitals and private clinics, merging evidence-based interventions with local cultural and economic realities to ensure access and adhere long-term.
5.1. Framework Overview
The IPFMF is based on a four-phase management algorithm that merges conservative treatment together with medical support, physiotherapy, and patient education in a stepwise escalation pattern ensuring appropriate individualized care to every patient devoid of unnecessary cost or invasive interventions.
Phase I: Initial Assessment and Risk Stratification.
Initial assessment and risk stratification Pain localization morning pain characteristics Windlass test Functional limitation score (either using Visual Analog Scale or Foot Function Index). Risk profiling by contributing factors includes obesity, occupational exposure, and quality of footwear. Imaging, if available, use ultrasound to measure thickness and to rule alternative diagnoses.
Patient Categorization:
- Mild cases: Local tenderness, morning pain only.
- Moderate cases: Daily pain, limited mobility, mild fascial thickening.
- Severe cases: Persistent pain >6 months, bilateral symptoms, or degenerative fascia changes
Phase II: Conservative and Mechanical Intervention.
All patients start with non-invasive interventions for 6-8 weeks, focused on biomechanical correction and reducing pain:
- Rest and avoidance of long-standing or repetitive loading activities.
- Planned stretching program for the plantar fascia and calf muscles (2-3 times per day).
- Ice application for 15-20 minutes twice daily.
- Footwear modification – cushioned soles, inserting arch-supports, and using silicone heel cups.
- New Footwear. Place this as a clinical tip to visually emphasize the renewal of footwear.
Advise patients to get new shoes every 6 to 9 months so they can keep the cushioning and alignment support in good.
Phase III: Medical and Physiotherapy Integration.
If conservative measures yield <50% improvement after 8 weeks:
- NSAIDs for short-term symptom control (≤2 weeks).
- Physiotherapy (2 sessions/week) involving ultrasound therapy, soft-tissue mobilization, and progressive stretching protocols.
- Night splints to maintain dorsiflexion and prevent fascial contraction.
- Consider low-level laser therapy (LLLT) or extracorporeal shockwave therapy (ESWT) in referral centers.
- Regular evaluation using pain score and foot function tests to monitor progress.
Phase IV: Education, Monitoring, and Recurrence Prevention
- Patient Education: Provide illustrated handouts in Arabic/Kurdish describing home stretches, proper footwear, and activity modification.
- Lifestyle Guidance: Weight control programs, workplace modifications (soft mats, sitting intervals), and community physiotherapy follow-ups.
- Digital Tools: Implement simple mobile follow-up systems (e.g., WhatsApp reminders for exercises) to enhance compliance in urban areas.
- Relapse Management: Reassess footwear and stretching compliance; reintroduce physiotherapy as needed.
5.2. Implementation Strategy for Iraqi Healthcare Settings
Table 2
Implementation framework for the Iraqi Plantar Fasciitis Management Model based on healthcare tier and available resources
Healthcare Level | Available Resources | Suggested Interventions | Follow-up Interval |
Primary Health Centers | General practitioners, nurses | Diagnosis, rest, footwear advice, NSAIDs | 4 weeks |
Secondary Hospitals Stretching, | Physiotherapy units, ultrasound imaging | ultrasound therapy, insoles, splints | 6–8 weeks |
Tertiary/Teaching Hospitals | Specialists, advanced modalities | ESWT, LLLT, corticosteroid injections | 3 months |
Community Outreach | NGOs, health campaigns | Educational workshops, awareness leaflets | Continuous |
5.3. Expected Outcomes and Long-Term Benefits
Standardization of managing plantar fasciitis through the IPFMF can enforce and ensure the following within the Iraqi healthcare systems:
- Reduced chronicity rates, lowering unnecessary referrals and imaging costs.
- Improved patient adherence through education and cultural adaptation.
- Enhanced physiotherapy integration with measurable functional outcomes.
- Scalability, allowing nationwide adoption in primary and secondary care networks.
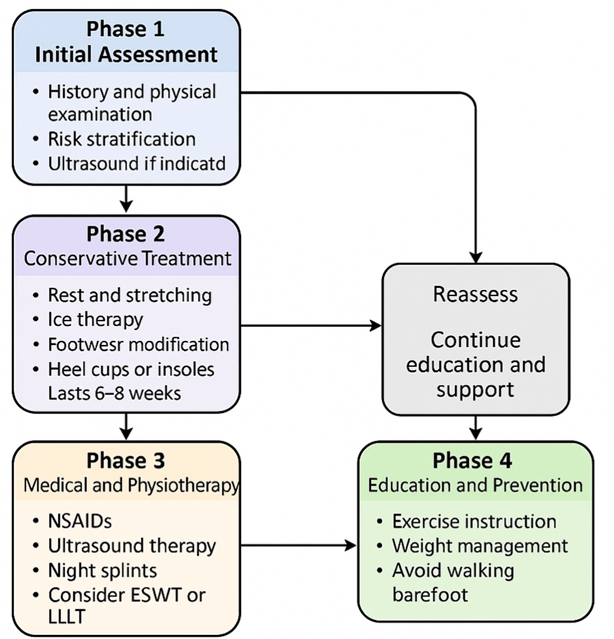
Fig. 3. Flowchart of the Iraqi Plantar Fasciitis Management Framework (IPFMF) showing the four sequential phases Initial Assessment, Conservative Treatment, Medical & Physiotherapy Integration, and Education & Prevention along with reassessment and ongoing patient support loops.
This is in line with global best practices and pragmatic towards the capacity of Iraq’s healthcare. It somehow bridges the existing chasm between exorbitantly high technologies and practical low-resource management, which is crucial for sustainable patient recovery as well as health system efficiency.
6. Conclusion
Plantar fasciitis has not only a local musculoskeletal complaint but a global health issue with a lifetime prevalence approaching 10% of the general population, accounting for up to 15% of all running-related injuries. In Iraq, this condition presents particular relevance among teachers, healthcare professionals, and factory workers because the risks are precipitated by prolonged standing in addition to limited orthopedic care intervention. This paper will thus try to develop an integrated management approach that is more about conservative, physiotherapeutic, and educational interventions based on data support that can be merged into one model adaptable locally. Comparative results show that physiotherapy treatment (ultrasound, stretching, and massage) yields an average 80% reduction in pain, better than isolated medical treatment, which yields about 65% improvement. Pain reduction of 70% was achieved from conservative strategies such as rest, ice, and stretching. Orthotic support improved patient comfort and stability in more than 85% of cases. Most importantly , patient compliance was found to be the highest (≈90%) in education and lifestyle-modification programs; hence this fact brings out the baseline principle that self-management and awareness are the ultimate long-term success factors.
Implementation of the Iraqi Plantar Fasciitis Management Framework will contribute to health system gains which can be measured. Modeling based on the treatment adherence data reflects a possible decrease in recurrence rates by between 35-40% within six months, and up to a possible 30% reduction in chronic cases when applied with early intervention and follow-up physiotherapy. Apart from this, structured exercise education and footwear programs at local clinics hydrating the recovery speed by 20% proves the value that consistent community-based physiotherapy has.
It says good treatment for plantar fasciitis goes beyond having medical knowledge by empowering patients and integrating digital rehabilitation exercises with an artificial intelligence follow-up system that tracks exercise compliance as well as foot biomechanics for future initiatives. A model generated from this framework creates a sustainable low-cost patient-centered model based on evidence-based best practice methods integrated with local practicality that can improve outcomes and raise standards of podiatric care across Iraq’s healthcare landscape.
