
Silent myocardial infraction (SMI) – transient dysfunction of perfusion, metabolism, function or myocard electrical activity, which is accompanied by anginal attack or its equivalent [2]. The main cause of both SMI and angina is arterial sclerotic disease of coronary arteries (CA). According to P.F. Cohn, angina, myocardial infraction or sudden death are further developed in 34% of patients. SMI raises the risk of sudden death by 10 times, arrhythmia – by 2 times, development of IM and congestive heart failure – by 1-1.5 times [11].
Coronary angiography has become a routine diagnostic method of CAD and helps to determine type, degree and distribution of lesion of coronary arteries [6]. One of the key factors, which determine prognosis of the patients with SMI, is incidence of atherosclerotic coronary bed lesion. At the same time, the data available in the literature about connection of SMI with the nature of obstructive lesion of coronary arteries are ambiguous.
The purpose of the study is detection of specific aspects of coronary artery disease in the patients suffering from CAD with concomitant type 2 diabetes mellitus according to coronary angiography data.
Documents and methods. Prospective analysis of 86 medical histories of the patients with SMI was conducted. The patients were undergoing treatment in cardiovascular care unit of the Hospital with clinical research center of cardiology and were examined by coronary angiography within the period from April 2020 to March 2022. All 86 patients, of which 74 men (86.0%) and 12 women (14.0%), were suffering from CAD with concomitant type 2 DM, aged from 30 to 71 (average age is 59.8±8.9). 46 patients (53.5%) had type 1 SMI, 40 patients (46.5%) – type 2 SMI. Duration of the disease was from 0.4 to 15 years, i.e. 5.3±1.5 on the average. The medical history of 33 (38.3%) patients with SMI contained a record of previous myocardial infarction. When analyzing comorbid diseases: 61 (70.9%) patients with SMI had high blood pressure, 38 (44.2%) patients had cardiac rhythm and conduction disorder. Coronary angiography was performed in the department of diagnosis X-ray surgery methods and treatment using “Artis Zee” device. In visual analysis of coronary angiograms, main coronary arteries were evaluated: Left main coronary artery (LMCA), right interventricular artery (RIVA), circumflex artery (Cx), right coronary artery (RCA). Presence of multiple arterial involvement and number of affected arteries were evaluated. All patients passed clinical laboratory examination.
Results and their discussion Analysis of lesion frequency of main coronary arteries based on the coronary angiography results showed that 6 (7.0%) patients had slightly affected CA, 13 (15.1%) patients had single-vessel coronary artery disease, 27 (31.4%) patients – two-vessel, 40 (46.5%) patients – multiple-vessel. Average number of affected CA in the patients amounted to 2.5. It was established that RIVA is affected in most cases – 74 (86.0%) patients (p>0.05), RCA – 25 (29.1%) patients, Cx – 17 (19.8%) patients, LMCA – 8 (9.3%). Herewith, hemodynamically relevant stenosis of RIVA averaged to 80.3±81%, Cx – 72.8±3.2%, RCA – 85.7±5.9% (fig.).
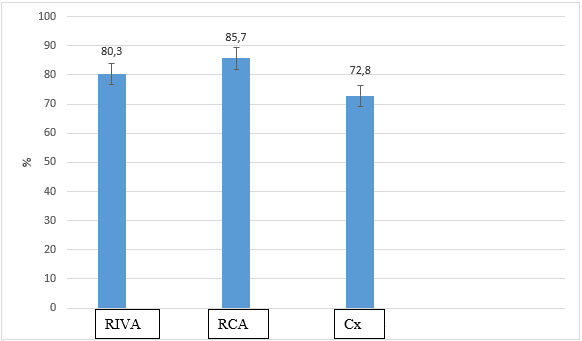
Fig. Lesion percent of main coronary arteries
Analysis of lesion level showed predominance of proximal and mid segments of RIVA (51.1% and 36.5% accordingly), RCA (44.0% and 24.0% accordingly), and Cx (35.3% and 47.1% accordingly). Hemodynamically relevant stenosis were observed in RIVA in 31 (41.9%) patients, RCA - 21 (84.0%) patients, Cx – 13 (76.5%) patients, LMCA - 5 (62.5%). In the analyzed group of patients, the most frequently affected second order coronary artery was obtuse marginal branch (OMB) – branch of LCA (32.5%), posterior descending coronary artery (PDA) – branch of RCA, and posterolateral branch (PLB) – branch of Cx (6.5%). Herewith, hemodynamically relevant stenosis in OMB were observed in 48.6% of cases; in 37.8% of cases lesion was observed in proximal compartment.
Some researchers believe that [9] in the patients with various clinical forms of CAD, the severity of coronary bed lesion is not the factor specifying presence or absence of SMI. However, other authors [7, 13] comparing lesions of CA in the patients suffering from painful myocardial ischemia (MI) with the patients suffering from SMI, marked these differences [4]. In comparison of the data of coronary angiography, close correlation between silent ischemia and severity of coronary atherosclerosis is observed. Herewith, the more coronary arteries are affected, the more episodes of SMI, both isolated and combined with MI, are observed [14].
Number of researchers discovered that in 50% of the patients suffering from CAD with SMI episodes, revealed at coronary angiography examination, there were significant arterial sclerotic lesion of proximal compartments of CA [10] and hemodynamically relevant stenosis [4,5]. When studying peculiarities of coronary bed lesion in the patients suffering from SMI, two-vessel coronary bed lesion was observed significantly more common (50%) than in the patients with effort angina. In the patients suffering from SMI, prevailing lesion of RCA (84.0%) over lesion of other CA was observed.
In addition, there are contradictory data about distribution of obstructive lesions of CA in the patients suffering from SMI or MI. Some studies showed that 92% of the patients suffering from SMI had lesions in proximal segments of CA [1, 10]. Another studies showed no differences in incidence or allocation of stenosis of CA in the patients suffering from CAD with IM or SMI. Herewith, it is noted that lesion of proximal compartments of CA in the patients suffering from SMI is observed less common – only in 50% of patients [12]. It should be emphasized that lesion of only one vessel differs not only by distribution, but also by degree of stenosis. Now, there are several opinions regarding correlation between frequency and duration of SMI episodes and degree of lesion manifestation of CA. Therewith, with increase of CA obstruction, the frequency of SMI episodes raises [14]. The authors showed that in the patients with one, two or three affected vessels and clinical pattern of SMI, the frequency of ST segment displacement was raising in the course of increase of duration of CA stenosis [15].
Therefore, the obtained analysis data of the results of coronary angiography in the patients suffering from SMI confirm the data of some studies that in the patients suffering from SMI the multiple lesions of CA are prevailing, RIVA is affected most frequently, mid and proximal segments are prevailing, the most frequently affected second order CA is OMB. Inconsistency of the available data on intensity of coronary artery disease in the patients suffering from SMI requires further study.
