
Introduction
Alopecia is defined as the absence of hair in an otherwise hairy area. There is typically little inflammation or scarring associated with diffuse hair loss. Hair thinning occurs in what appears to be a random pattern over the scalp. The effects of several nutritional illnesses on hair show that it, like other organs, need proper nourishment. Significant hair changes are a symptom of protein energy deficiency in particular. Many different micronutrients have been suggested as potential causes of hair loss in addition to Protein–energy malnutrition (PEM) [1].
Human hair not only contributes to a man's psychological health, but it also serves a defensive purpose. It shields the skin from the sun's rays, which can cause cutaneous cancer if you have a bald head. The arrector pili muscle is flexed in a protective manner to keep the cold out. The hair shaft also transfers cellular debris out of the follicular canal and helps spread sebum, sweat, and odors throughout the skin's surface. The outer root sheath in the hair follicle bulge is rich in stem cells. Damage to the epidermis and a halt in hair follicle and sebaceous gland development occur when hair follicle stem cells are depleted [2].
With regard to hair loss due to the rise in the prolactin hormone, there is not much research on this thing. Therefore, a number of studies have been collected in order to know whether the prolactin hormone has an effect on hair loss.
The pituitary gland, located at the of the brain, is responsible for producing the hormone prolactin. The mammary glands aren't the only organ that produces the hormone; the brain, the immune system, the skin, the uterus, and so on all contribute. [3] Among its many uses is stimulating lactation in the breasts after giving birth. Therefore, an increase in prolactin is to be expected during pregnancy and breastfeeding. In addition to encouraging lactation, it plays a key role in metabolic regulation, fluid homeostasis, and immune system function [4].
Researchers have found that male-pattern baldness (androgenic alopecia) and other forms of hair loss can be triggered by hyperprolactinemia. For instance, one German study linked hair loss, PMS, seborrhea (excessive release of sebum from sebaceous glands), and chronic acne to hyperprolactinemia [5].
Fewer than a handful of articles have addressed hair loss and hyperprolactinemia in women in the medical literature in the previous 30 years. Therefore, 40 women with diffuse alopecia were tested for hyperprolactinemia to determine its significance.
Lutz G. 2012 Clinicians and pluck trichograms assessed hair loss. 17.5% of women experienced androgenetic alopecia and 82.5% diffuse hair loss. Prolactin levels reached 1390 and 255 ng/ml. Six individuals had 150–80.4 ng/ml and 10 had 79.1–51.7. All others had prolactin ≤ 50 ng/ml. 15 untreated prolactin-elevated patients may be monitored. Reductions, normalizations, and modest variations were observed without prolactin-inhibiting medications [6].
Zvonimir Bosnić et al., 2021 95% of thyroid-specific tests were normal. 2.5% exhibited minor hyper- and hypothyreoidism. All female patients had normal testosterone, androstendione, and dihydroepiandrostendione levels.
These findings suggest that moderate increased prolactin in androgenic or widespread alopecia do not affect the pattern, amount, or duration of the hair loss. Other scientists found only high levels of prolactin inhibited human hair follicles in vitro. However, moderate consistently increased prolactin levels should prompt pituitary gland tumor testing.
General practitioners, who are the first to diagnose and treat hair loss in women, face many hurdles. Endocrine abnormalities, pharmacological side effects, and stress are often secondary causes. We propose a putative pathophysiological relationship between hyperprolactinemia and baldness in a preexisting autoimmune thyroid condition. A 27-year-old woman on hormone replacement treatment for autoimmune thyroid disease presented to a family doctor with frontal alopecia that had started months previously. Diagnosis: frontal alopecia. Thyroid ultrasonography and lab testing confirmed autoimmunity. Her hormones were normal. Due to high prolactin, pituitary gland computed tomography ruled out brain pathology. No large cohort studies have examined hyperprolactinemia-induced baldness in autoimmune disorders. This report suggests that moderately increased prolactin results require further investigation to rule out a pituitary gland tumor [7].
TUĞRUL et al., 2021 Prolactin's effects on hair follicles and hair loss are still debated. This study examines female telogen effluvium patients' serum prolactin levels and hair loss. Materials and methods: This retrospective analysis comprised 47 adults female telogen effluvium patients and 42 age-matched healthy controls. Telogen effluvium patients and healthy controls were compared for serum prolactin (Mann-Whitney U test). Results: The median patient age was 29 (19-46) years and the median symptom duration was 12 (1-156) months. Neither patients nor controls had hyperprolactinemia. Patients had a median serum prolactin level of 10.47 ng/mL (2.75-23.53), substantially lower than controls (p=0.033). Acute and chronic telogen effluvium patients had similar prolactin levels (p=0.444). Conclusion: Unlike most research that show prolactin induces catagen, our study reported lower prolactin levels in telogen effluvium patients than controls. However, most studies linking hyperprolactinemia with hair loss include hyperandrogenemic individuals and describe high levels of prolactin's catagen-inducing impact. Hyperprolactinemia and hyperandrogenism were absent in this study, which may explain the discrepancy. Thus, the dose and gender-dependent effects of prolactin on hair loss may be informative [8].
In 1989. Thirty-one women with androgenetic alopecia were examined for hypothyreoidism and hyperprolactinemia using the TRH test. In 7 cases (23%), TRH stimulation raised TSH levels, indicating hypothyreoidism. After TRH stimulation, 9 individuals (29%), had hyperprolactinemia. Prolactin stimulates suprarenal gland cortisol and testosterone synthesis, hence it was given special attention. Low thyroxin and high prolactin levels disrupt androgen metabolism, causing female pattern baldness. The team's subsequent research in a larger patient sample supported the theory that prolactin's androgen-stimulating effect causes female-pattern baldness [9].
What is Hyperprolactinemia?
Prolactin levels in the blood are increased in a condition known as hyperprolactinemia. Prolactin is a hormone that increases the production of breast milk and has an impact on both men and women's levels of the sex hormones estrogen and testosterone.
What is Prolactin?
Acidophilic cells called lactotropes in the anterior pituitary gland secrete the peptide hormone prolactin. Dopamine inhibitory tone primarily controls how much is secreted by the anterior pituitary. The hypothalamic hormone TRH, whose major function is to control the production and secretion of TSH from the pituitary, does, however, have a slight stimulatory influence on prolactin release.
What are symptoms of Hyperprolactermia in both sexes?
- Breast discharge and breastfeeding, Low levels of other pituitary hormones; Infertility, Reduced libido, Headaches, Visual abnormalities, Bone loss (osteoporosis) and loss of vision.
Hyperprolactinemia Symptoms in Females
- Vaginal dryness, Pain during sex, an irregular menstrual cycle or amenorrhea (no periods), Breast milk production while not nursing or pregnant, Acne and excessive body and facial hair development.
Hyperprolactinemia Symptoms in Males
- Breast enlargement; low testosterone; difficulty obtaining or maintaining an erection; decreased muscular mass or body hair.
What are causes Hyperprolactinemia?
There are numerous causes of increased prolactin levels. The most frequent causes are pregnancy and breastfeeding, when prolactin levels are naturally and as they should be raised. Yet occasionally, factors like exercise, starvation, stress, medicine, or a medical condition might affect how well the pituitary functions.
Aside from pregnancy and lactation, causes of elevated prolactin levels include:
- Hypothyroidism (underactive thyroid, in which the thyroid gland does not produce enough thyroid hormone).
- Chronic liver or kidney disease.
- Nipple stimulation.
- A growth or tumor on the pituitary gland. Prolactinomas, growths or tumors on the pituitary gland that cause prolactin levels to be high, are usually benign. When the tumors are larger than 1 centimeter, they’re called macroprolactinomas. These can cause headaches and issues with vision.
- Injuries or conditions that affect the chest wall.
- Hormone Health Network (from the Endocrine Society). Hyperprolactinemia. Last Updated April 2020. Accessed December 15, 2021.
- The Mayo Clinic. Prolactinoma No Date. Accessed December 15, 2021.
- Journal of Human Reproductive Sciences. 2013. Hyperprolactinemia Accessed December 15, 2021.
How is Hyperprolactinemia Tested?
Before beginning any treatment, it is important to obtain a comprehensive clinical history in order to make an accurate diagnosis of hyperprolactinemia. Before the problem is diagnosed, physiological causes, systemic disorders, and the usage of specific drugs must be ruled out. Asymptomatic individuals and those with increased prolactin without a known reason should be screened.
Prolactin blood levels are frequently checked in men with decreased sexual function and milk secretion as well as in women with unexplained breast milk secretion (galactorrhea), irregular menstrual cycles, or infertility. All known diseases and drugs that increase prolactin secretion must be evaluated and ruled out for diagnosis if high prolactin levels are observed. TSH levels are evaluated if prolactin levels are still high after ruling out all other potential explanations. If TSH levels are high, hypothyroidism is the primary cause of hyperprolactinemia, and it should be treated as such.
An MRI or CT scan is performed to check for any pituitary adenomas if TSH levels are normal. Prolactinomas found in postmenopausal women are often macroadenomas, despite the fact that hyperprolactinemia is frequently uncommon in this population. Little microadenomas won't be visible on a simple X-ray of the bones surrounding the pituitary, despite the presence of a huge macroadenoma. The most accurate diagnostic for locating and measuring pituitary tumors is magnetic resonance imaging (MRI). Repeated MRI scans may be used to monitor the development of the tumor and the impact of treatment. The pituitary gland can also be seen on a CT scan, albeit it is less sensitive than an MRI in detecting abnormalities in pituitary gland size. Physicians evaluate the size of the pituitary tumor in addition to inspecting the surrounding tissues for damage and running tests to determine whether the production of other pituitary hormones is normal. Doctors may ask for an eye exam that involves the measuring of visual fields depending on the size of the tumor.
Women's hair loss is a growingly common issue. Depending on the cause, the clinical features of female pattern hair loss vary. When a woman has typical female androgenetic alopecia (FAGA), the problem begins with a specific diffuse loss of hair in the parietal or frontovertical areas ("in the crown") while still preserving the frontal hairline. The woman needs assurances that the hair loss won't last forever.
Reaches total alopecia, but her hair's diameter will gradually get thinner as well as finer, shorter, and depigmented, allowing the scalp to be visible. This process, which Erick Ludwig called "rarefaction," describes how female alopecia progresses from uniform shrinking of the hairs in the centroparietal areas, or "crown," to diffuse alopecia with an oval shape and a zone of hair with normal density surrounding it. The width of this band varies depending on the region; in the frontal region, it is 1 cm to 3 cm, in the temporoparietal areas, it is a little wider, between 4 cm and 5 cm, and in the occipital region, the alopecia is separated from the normally hairy occipital zone by a broad line that runs between the vertex and occipital area. The frontal hairline condition is always maintained in FAGA, unlike fully established MAGA (male androgenetic alopecia), or "Hippocratic alopecia," and there are no elevations in blood biochemical levels.
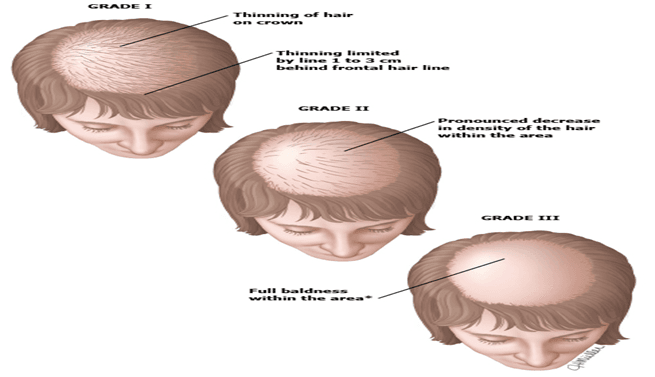
Fig. The classification of Ludwig. Loss of hair progresses via three stages. Adapted from Ludwig et al. with their permission
Does Prolactin Cause Hair Loss?
The truth is that a connection between prolactin and hair growth has yet to be established by science.
Because there is no proof that prolactin levels promote hair loss in women, this theory has been rejected. Yet, it was still recommended that women with elevated prolactin levels, or hyperprolactinemia, be watched over time, if only for study.
Prolactin may have a mechanism for interrupting the hair growth cycle and forcing follicles into the catagen phase, which suggests that prolactin may be a risk factor for telogen effluvium. This theory is supported by research that suggests prolactin may be a contributor to the larger issue of androgenetic alopecia.
A 2004 study that examined 37 males who had premature androgenic alopecia to see if they had elevated prolactin levels discovered a "borderline trend" of relevance between those prolactin levels and premature hair loss in this small sample size.
The study failed to come to any conclusions on a causal link between prolactin and hair loss.
Only a few articles on hair loss and hyperprolactinemia in women have been published in the past 30 years' worth of research, while a causal connection is more frequently discussed. The types of hair loss associated with hyperprolactinemia are primarily of the diffuse or androgenetic variety and are linked to hormonal anomalies, particularly androgens.
A 2012 study examined Our findings suggest that moderately high prolactin levels in diffuse or androgenetic hair loss can be disregarded as a potential hair loss cause since there is no proof that they have an impact on the pattern, severity, or duration of the hair loss. Investigations by other writers who only described an inhibitory impact of prolactin at high dosages provide support for these findings.
